
Liver transplantation is a life-saving procedure, but it also marks the beginning of a new chapter—one filled with recovery, resilience, and adjustment to a ‘new normal.’ While the transplant offers a second chance at life, it comes with its own set of post-liver transplant complications that patients and caregivers must be prepared for.
From managing immunosuppressant medications to being vigilant about signs of infection or rejection, this journey requires awareness and proactive care. But it’s not just about medical vigilance—it’s also about embracing a lifestyle that prioritises well-being, emotional balance, and long-term health.
💡 Before You Scroll Further… Let’s Share Some Stories
🧕 Sarita’s Story – A Silent Storm
She had just returned home, post liver transplant.
Her family was celebrating — finally, some relief.
But within weeks…
Fatigue.
Low-grade fever.
Mild tummy discomfort.
Everyone thought it was “normal post-surgery stuff.”
Until she worsened.
Diagnosis?
Biliary sepsis — a hidden complication most patients don’t see coming.
Sarita recovered, but the scare taught her and her caregivers:
Transplant isn’t the end. It’s the beginning of vigilant care.
👨🦳 Keshav’s Journey – When the Liver Fought Back
Six months after his transplant, Keshav felt… fine.
Stable vitals. Regular meds. Good appetite.
But then came the yellow eyes.
The itching.
And that eerie sense of déjà vu.
A routine test revealed the truth:
Rejection.
Not due to missed meds.
Not due to negligence.
Just… the body being unpredictable.
With prompt treatment, he stabilised again.
But Keshav now knew —
A transplant is a team effort that never truly ends.
In this comprehensive guide on common post-liver transplant complications: what to expect and when to worry, we walk you through the most frequent issues faced by both recipients and donors. You’ll learn how to recognise early warning signs, understand why certain complications occur, and discover how modern medicine and compassionate care make most of these challenges manageable.
Importantly, this post isn’t just about risks—it’s about reassurance. Life after liver transplant can be vibrant, purposeful, and fulfilling. Many patients return to work, enjoy family life, and take on meaningful activities—sometimes with even greater clarity and gratitude than before. The key lies in being informed, consistent with follow-up care, and emotionally supported.
Whether you’re a patient, a loved one, or a caregiver, this post is here to offer clinically accurate, clear, and compassionate information to help you navigate the post-transplant path with confidence and hope.
🎙️Podcast: Post-Liver Transplant Complications
Risk Factors for Post-Liver Transplant Complications
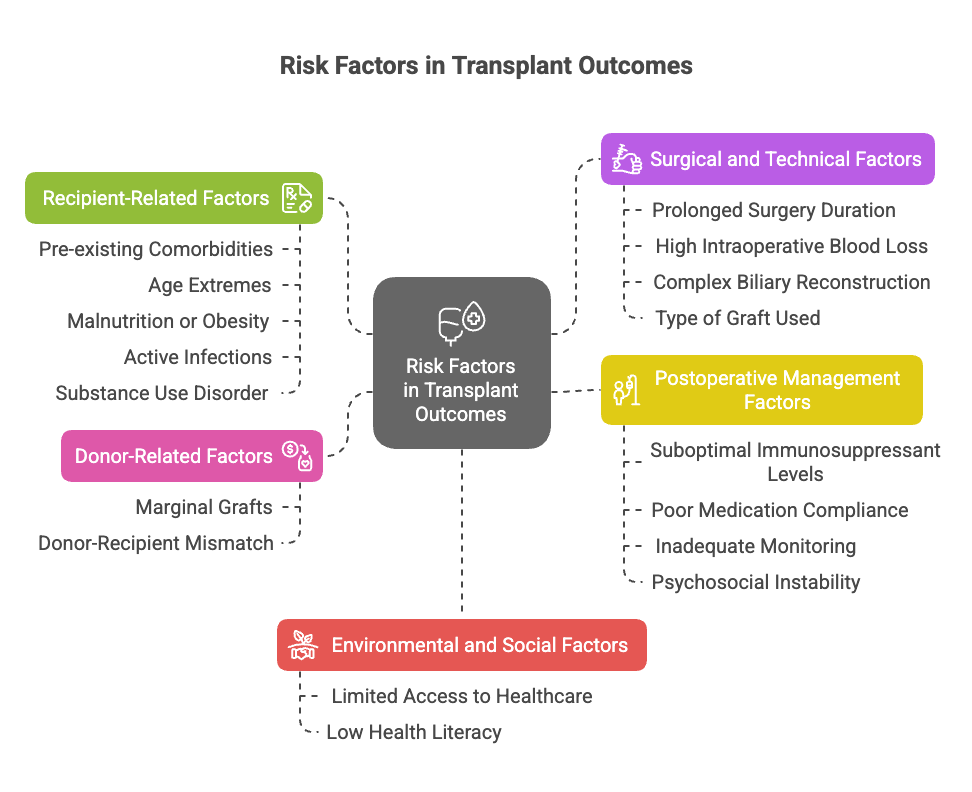
Identifying risk factors early helps optimise outcomes and personalise follow-up care. These risk factors apply to both recipients and, where relevant, to donors:
1. Recipient-Related Factors
- Pre-existing comorbidities: Diabetes, hypertension, chronic kidney disease, and cardiovascular disease increase postoperative morbidity.
- Age extremes: Pediatric and elderly patients have unique vulnerabilities due to immune status and physiological reserves.
- Malnutrition or obesity Alters wound healing, immunity, and drug pharmacokinetics.
- Active infections at time of transplant: Latent infections like CMV, EBV, TB, or fungal infections can flare post-transplant.
- Alcohol or substance use disorder: Increases risk of non-compliance, liver injury recurrence, and complications.
2. Surgery-related Factors
- Prolonged surgery duration: Correlates with higher infection and vascular complication rates.
- High intraoperative blood loss or transfusion requirement: Increases immunologic sensitisation and infection risk.
- Complex biliary reconstruction raises the chances of bile leaks and strictures.
- Type of graft used: Living donor, split-liver, or marginal donor grafts may have varying complication risks.
3. Postoperative Factors
- Suboptimal immunosuppressant levels: Can lead to rejection (if low) or infections/toxicity (if high).
- Poor medication compliance: A major preventable cause of rejection.
- Inadequate monitoring or follow-up: Delays the detection of early complications like vascular stenosis or drug toxicity.
- Psychosocial instability: Depression, anxiety, or lack of family support impact recovery and medication adherence.
4. Donor-Related Factors (For recipients)
- Marginal grafts: Elderly donors, fatty liver, or prolonged ischemia times raise the risk of primary graft dysfunction.
- Donor-recipient mismatch: Size mismatch, ABO incompatibility (even with desensitisation), can lead to complications.
5. Social Factors
- Limited access to healthcare or transplant centres, especially in rural areas, affects early complication detection.
- Low health literacy: Patients may not recognise red flags or understand medication importance.
For the Recipient: Key Complications You Might Face
38% of deceased donor liver recipients and 47% of living donor liver recipients experienced a complication within 90 days of transplant. Biliary, hemorrhagic, and vascular complications were significant sources of morbidity and mortality.

1. Rejection of the Liver Graft
Rejection occurs when the body’s immune system attacks the new liver. It can be acute or chronic.
Ductopenia: The loss of bile ducts, a feature of chronic rejection.
Diagnosis requires a liver biopsy.
Symptoms: Fatigue, jaundice (yellowing of eyes/skin), dark urine, abdominal pain, or fever.
Management:
- Early rejection is usually manageable.
- Diagnosis: Liver function tests (LFTs), liver biopsy if required.
- Treatment: High-dose steroids (e.g., methylprednisolone bolus), adjusting immunosuppressant doses, sometimes switching medications.
- Reassurance: With timely detection and treatment, most patients recover well from rejection episodes.
2. Infections (Bacterial, Viral, Fungal)
Pre-transplant screening for various infections (bacterial, fungal, viral) is crucial to prevent recrudescence under immunosuppression.
Common types: Pneumonia, urinary tract infections (UTIs), CMV, fungal infections like candidiasis.
Symptoms: Fever, chills, breathing difficulty, burning urination, general malaise.
Management:
- Blood/urine/sputum cultures, imaging (e.g., chest X-ray)
- Prompt admission may be needed.
- Antibiotics/antivirals/antifungals are given based on the organism identified.
- Prevention with vaccines, hygiene, masks, and timely reporting of symptoms.
- Reassurance: Most infections are treatable if caught early.
3. Biliary Complications
Biliary complications (BCs) are the most common complications after LT, with an incidence ranging from 10% to 19%. The most frequent types are anastomotic stricture.
- The three most common types of biliary complications after liver transplantation are anastomotic strictures, nonanastomotic strictures, and biliary leaks. These can occur at various times post-transplant.
- Significant risk factors for biliary complications include preoperative hyponatremia, advanced liver disease, underlying conditions like primary sclerosing cholangitis or malignancy, donor factors (age > 60, graft steatosis), surgical factors (techniques, graft type, ischaemia time), and post-LT complications like HAT or CMV infection.
- LDLT is associated with a higher incidence of Biliary complications and more challenging strictures due to smaller graft size, smaller donor duct calibre, and potentially multiple anastomoses.
- Machine perfusion (MP) techniques have been promising in the prevention of the development of post-Liver Transplant Biliary Strictures.
- Anastomotic strictures typically present within the first year after LT, while nonanastomotic strictures usually present later, with a median time of 6 months but frequently appearing at 1 year or even 10 years post-LT.
Symptoms: Fever, jaundice, abdominal pain, or raised LFTs.
Management:
- Imaging: Ultrasound, MRCP.
- Procedures: ERCP with stenting, percutaneous drainage for bilioma.
- In some cases, repeat surgery may be required.
- Reassurance: These are among the most common and treatable issues post-transplant.
4. Kidney Dysfunction
Pre-existing renal dysfunction in the recipient is a major risk factor. Other factors include metabolic syndrome (diabetes, hypertension, obesity), particularly in patients with NASH/MAFLD, and possibly aspects of immunosuppression.
Symptoms: Swelling, reduced urine output, high creatinine.
Management: Management involves addressing underlying risk factors like hypertension and dyslipidemia, and careful management of immunosuppression.
- Dose adjustment of medication
- Renal consult
- Switching to kidney-friendly alternatives
- Reassurance: Regular monitoring helps catch changes early and prevent long-term damage.
5. Recurrence of Original Liver Disease
At-risk patients:
- Hepatitis B or C
- Alcoholic liver disease
- Hepatocellular carcinoma (HCC)
Management:
- Regular follow-up labs, imaging
- Antiviral therapy for hepatitis
- Abstinence support for alcohol-related disease
- Surveillance protocols for HCC recurrence
- Reassurance: With regular monitoring, these can often be kept under control or detected early.
6. Vascular Complications (thrombosis or stenosis)
- Various vascular complications can occur after liver transplantation, including hepatic artery thrombosis, hepatic artery stenosis(0.8%-10% incidence), and portal vein thrombosis.
- Risk Factors: Technical mistakes, damage to the endothelium, prolonged cold ischaemia time, recipient hypercoagulability, blood transfusions, transplantation in low-volume centres, and donor factors (age) are risk factors for HAT. Male sex is a risk factor for portal vein complications.
- There are potential consequences on the liver graft, and the typical diagnostic and management strategies for each Hepatic artery thrombosis (HAT) are the blockage of the hepatic artery, which is critical because it exclusively supplies blood to the bile ducts. HAT can lead to biliary ischaemic lesions, necrosis, and potentially graft failure.
- Symptoms: Deteriorating liver function, ascites.
- Management: Doppler studies, angiography may be required to confirm the diagnosis. Anticoagulation, sometimes surgical or radiological interventions. Early detection is crucial.
7. Medication Side Effects
- Symptoms: Tremors, diabetes, hypertension, gum swelling, weight gain.
- Management: Lifestyle modifications, dose titration, switching drugs if needed.
8. Metabolic Syndrome & Cardiovascular Risk
Metabolic syndrome (MS): A cluster of conditions (hypertension, obesity, high triglycerides, low HDL, high fasting blood glucose) that increase the risk of heart disease, stroke, and diabetes. It is a potential longer-term complication post-LT.
- Management: Early dietary guidance, lifestyle changes, and regular lipid/glucose checks are crucial.
9. Bone Health
- Long-term steroid use can affect bone density, leading to osteopenia or osteoporosis.
- Management: Vitamin D and calcium supplements, along with periodic DEXA scans, help maintain bone health in post-transplant survivors.
10. Malignancy Monitoring Post-Transplant
- Immunosuppression can increase the risk of certain cancers. Patients should be screened regularly for skin cancers, cervical cancer (in women), and lymphoproliferative disorders.
- Management: Sun protection, HPV vaccination, and annual checkups are part of routine long-term care.
11. Psychiatric and Emotional Challenges
Includes: Depression, anxiety, PTSD, sleep disturbances.
Causes:
- Steroid-induced mood changes
- Psychological burden of chronic illness
- Fear of recurrence
Management:
- Counselling/therapy
- Medication if needed (SSRIs, sleep aids)
- Peer support groups, mindfulness, and family involvement
- Reassurance: Mental health is an important part of transplant recovery and can be improved.
Mental Health Follow-Up
Regular psychological follow-up is not a luxury; it’s a necessity. The latest guidelines recommend routine depression and anxiety screening, especially in the first 12–24 months post-transplant, where the mental health burden is highest.
12. Graft vs Host Disease (GVHD) (very rare but fatal)
GVHD occurs when immune cells from the donor liver begin to attack the recipient’s tissues. While common in stem cell or small bowel transplants, it is extremely rare after liver transplantation, but when it does occur, it is life-threatening.
👀 Symptoms to RRecogniseEarly:
- Sudden onset of rash (may spread rapidly)
- Severe diarrhea
- Liver dysfunction (jaundice, worsening LFTs)
- Pancytopenia (drop in all blood cell lines)
- Fever, weakness, and rapid clinical decline
🛠️ Management:
- Immediate hospitalisation is essential
- High-dose steroids are the first-line treatment
- Biologic agents (e.g., anti-TNF, anti-IL-2 therapies) may be used in refractory cases.
- Supportive care in ICU: infection control, transfusions, nutrition, etc.
⚠️ Prognosis:
- Despite aggressive treatment, GVHD after liver transplant has a very high mortality rate.
For the Donor: What to Know and When to Worry?
Living liver donation has risks. Common complications include bile leak/biloma (9.2%), incisional hernia (5.6%), and infections (12.5%). Psychological difficulties are also reported.

1. Wound Infection or Seroma
- Generally mild and self-limiting.
- Management: Antibiotics, wound care, drainage if required.
2. Bile Leak or Stricture
- Incidence: Rare, but possible.
- Management: ERCP with stenting. Most donors recover fully.
3. Incisional Hernia
- Symptoms: Bulge at incision site.
- Management: Surgical repair if needed.
4. Psychological Concerns
- Feelings: Guilt, anxiety, mood changes.
- Management: Psychological counselling, peer support.
Most donors return to full health and resume normal life within 6–12 weeks.
Red Flag Symptoms Cheat Sheet
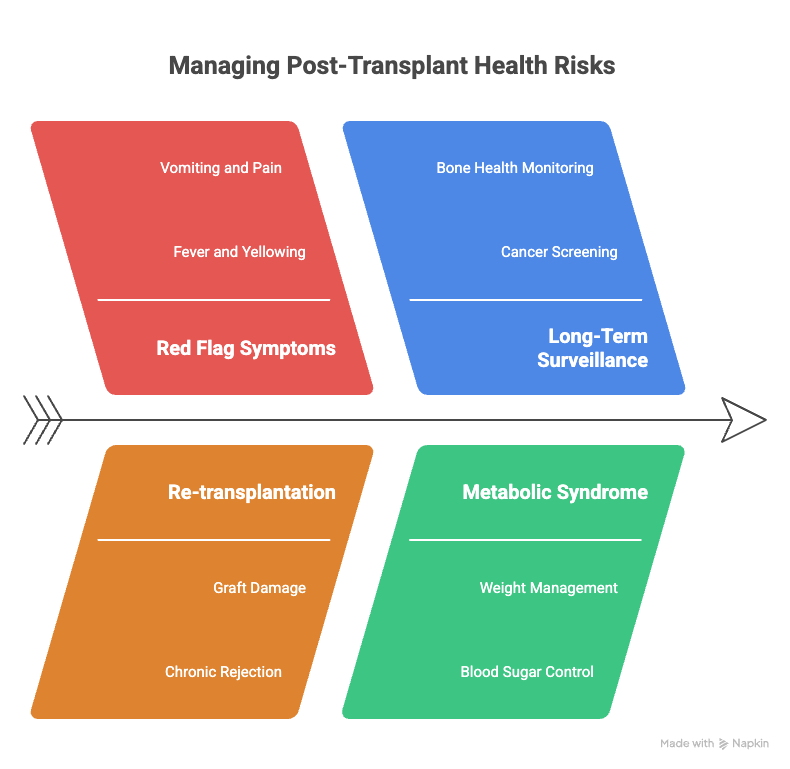
- Fever >101°F
- Yellowing of eyes or skin
- Persistent vomiting or abdominal pain
- Swelling at the incision site
- Breathlessness
- Blood in stool or black tarry stool
- Decreased urine output
- New onset of confusion or seizures
- Take Action: Contact your transplant team or go to the nearest emergency department. Don’t wait.
- Re-transplantation may be required in cases of irreversible graft damage, chronic rejection, severe complications, or disease recurrence. Up to 9% of liver transplant patients may require a second transplant.
- Long-Term Surveillance Strategies: Long-term surveillance is essential even years after transplant. According to recent guidelines, liver transplant recipients should undergo regular screening for malignancies (skin, colon, and post-transplant lymphoproliferative disorder), bone health monitoring, and metabolic syndrome management. This ensures longevity and improves quality of life.
📥 Download: Red Flag Symptoms After Liver Transplant — Cheat Sheet
FIB-4 Index Calculation in Post-Liver Transplant Monitoring:

📊 FIB-4 Index Calculator
Enter the values below to calculate the FIB-4 index for liver fibrosis.
Note: Check this link to know more about the interpretation of the score and FIB-4 Index https://livertransplanthelp.com/fib-4-index-calculator/
The FIB-4 index is a valuable tool for monitoring liver fibrosis in post-liver transplant patients, particularly those at risk of recurrence from infections like Hepatitis C (HCV) or other liver diseases such as NASH, alcohol-related liver disease, or autoimmune hepatitis. By using this non-invasive scoring system, clinicians can track the progression of liver fibrosis over time and assess the risk of advanced fibrosis or cirrhosis. In cases where FIB-4 scores are elevated, further diagnostic steps, such as a liver biopsy, may be considered. This scoring system plays a crucial role in guiding treatment decisions and helping to predict liver-related outcomes post-transplant, making it an essential part of ongoing care for transplant recipients, especially those with underlying liver conditions that may recur.
Final Reassurance:
You’re Not Alone
Liver transplantation is more than a surgical milestone—it’s the beginning of a new normal life filled with both renewed hope and complex challenges. While the procedure itself is life-saving, post-liver transplant complications—particularly biliary and vascular issues—are among the most common and impactful hurdles in the recovery journey.
Thanks to ongoing advancements in surgical techniques, imaging modalities, and postoperative care, many of these complications are now better managed than ever. Yet, they remain a persistent challenge that can significantly affect patient outcomes and quality of life.
Biliary complications, such as strictures or leaks, and vascular issues, including hepatic artery thrombosis, are key concerns that often require timely intervention. Their occurrence varies depending on factors such as whether the transplant was from a living donor or deceased donor, as well as the presence of pre-existing liver conditions and post-transplant immune responses.
To improve outcomes, there is a growing emphasis on personalised care plans, tailored according to patient risk profiles. Cutting-edge research is also exploring the role of machine perfusion techniques in preserving donor livers and minimising early complications.
Ultimately, understanding and managing post-liver transplant complications is not just about clinical survival—it's about empowering patients and caregivers to thrive in their “new normal” with confidence, clarity, and continuous care.
Facing complications doesn’t mean failure.
These are known challenges — with known solutions.
Your transplant team is trained to spot and manage them early.
🔑 The key is awareness.
🎯 The goal is trust + timely action.
💚 Stay informed. Stay strong.
You've already come so far — and you're not alone.
💬 Need Expert Guidance?
Want to talk to a doctor who’s walked this journey with hundreds of liver transplant patients?
Book a 1:1 Call with Dr. Tanuja Mallik
📚 Explore our curated resources: eBooks, recovery guides, and more.
This blog is part of the Dr. Tanuja Mallik Wellness Venture.
Created with compassion. Guided by experience.
Frequently Asked Questions
What is liver transplantation, and why is it performed?
Liver transplantation (LT) is a surgical procedure that replaces a diseased or failing liver with a healthy liver, or a portion of one, from either a deceased or living donor. It is considered the primary treatment option for individuals with end-stage chronic liver disease that cannot be managed with other therapies, as well as in rare instances of sudden liver failure.
The liver is a vital organ responsible for numerous functions, including processing nutrients, producing bile for fat absorption, creating proteins for blood clotting, removing toxins, and regulating immune responses.
What are some common indications for liver transplantation?
The most common indications for liver transplantation are chronic and acute liver failure, with cirrhosis accounting for approximately 80% of cases. Cirrhosis is frequently caused by chronic hepatitis C virus (HCV) infection, which is also a risk factor for hepatocellular carcinoma (HCC), a potential indication for LT.
Other indications include certain inherited metabolic diseases like primary hyperoxaluria type 1 and familial amyloid polyneuropathy, and in some cases, specific liver malignancies within clinical trials.
How are organs preserved for liver transplantation?
Organ preservation techniques are crucial to minimise damage before transplantation. Static cold storage (SCS) has been the traditional method. More advanced techniques, such as ex-situ machine perfusion procedures like normothermic machine perfusion (NMP) and hypothermic oxygenated machine perfusion (HOPE), are being explored.
These techniques aim to improve organ viability, expand the donor pool (including organs from older donors), provide time for better donor-recipient matching, and allow for assessment of organ function. In situ preservation methods, such as normothermic regional perfusion (NRP), also help reduce ischaemic damage by providing oxygen and nutrients to the liver before retrieval.
What are the major types of complications that can occur after liver transplantation?
Complications after liver transplantation can be categorised into surgical and medical complications. Major categories include vascular complications (such as hepatic artery thrombosis and stenosis), biliary complications (like strictures and leaks), and infections.
These complications can significantly impact postoperative morbidity and mortality rates.
What are the common vascular complications after liver transplantation?
Vascular complications, while having a global incidence of around 7%, are associated with high graft loss and mortality if not diagnosed and treated promptly. The most frequent arterial complication is hepatic artery thrombosis (HAT), which can occur early (within 30 days) or late.
HAT is a leading cause of graft loss and can lead to graft ischaemia, bile duct necrosis, and multi-organ failure. Hepatic artery stenosis (HAS) is less common but can lead to HAT if untreated. Other less frequent vascular complications include hepatic artery pseudoaneurysms and rupture, portal vein thrombosis and stenosis, and deep vein thrombosis and pulmonary embolism.
What are the common biliary complications after liver transplantation?
Biliary complications are relatively common, with incidences ranging from 2% to 19%. The most frequent are biliary leakage and biliary strictures. Extrahepatic biliary strictures, often occurring within the first year, can be caused by factors such as oedema, arterial complications (like HAT or HAS), and infection.
Intrahepatic biliary strictures, also known as ischemic-type biliary strictures, are more serious and often require retransplantation. Risk factors for biliary complications include donor characteristics, surgical technique, and graft preservation methods. Machine perfusion techniques, particularly HOPE and NMP, show promise in reducing the incidence of ischaemic-type biliary strictures.
What infectious complications are a concern after liver transplantation?
Infections are a significant concern after liver transplantation due to the immunosuppressive regimen recipients receive. Patients are screened for various bacterial, fungal, and viral infections before transplantation, including HIV, hepatitis A, B, and C, CMV, Mycobacterium tuberculosis, EBV, HHV-8, VZV, HSV, and Toxoplasma gondii.
Specific infections, such as aspergillosis, require effective treatment before LT. Cytomegalovirus (CMV) infection and post-transplant lymphoproliferative disorder (PTLD), often associated with Epstein-Barr virus (EBV), are notable viral complications that are closely monitored and managed.
What are the risks and considerations for living liver donors?
Living liver donation involves surgically removing a portion of a healthy person's liver for transplantation. While it offers the significant benefit of providing a life-saving organ and expanding the donor pool, it carries inherent risks for the donor. Potential complications for donors include biliary leaks, bacterial infections, incisional hernia, pleural effusion, neuropraxia, the need for reoperation, wound infections, intra-abdominal abscess, and vascular complications such as portal vein or inferior vena cava thrombosis.
Donors undergo a comprehensive evaluation, including physical and psychological assessments, medical history review, and diagnostic and imaging tests, to ensure they are in excellent health and understand the risks involved. The decision to donate should be made freely without pressure.